



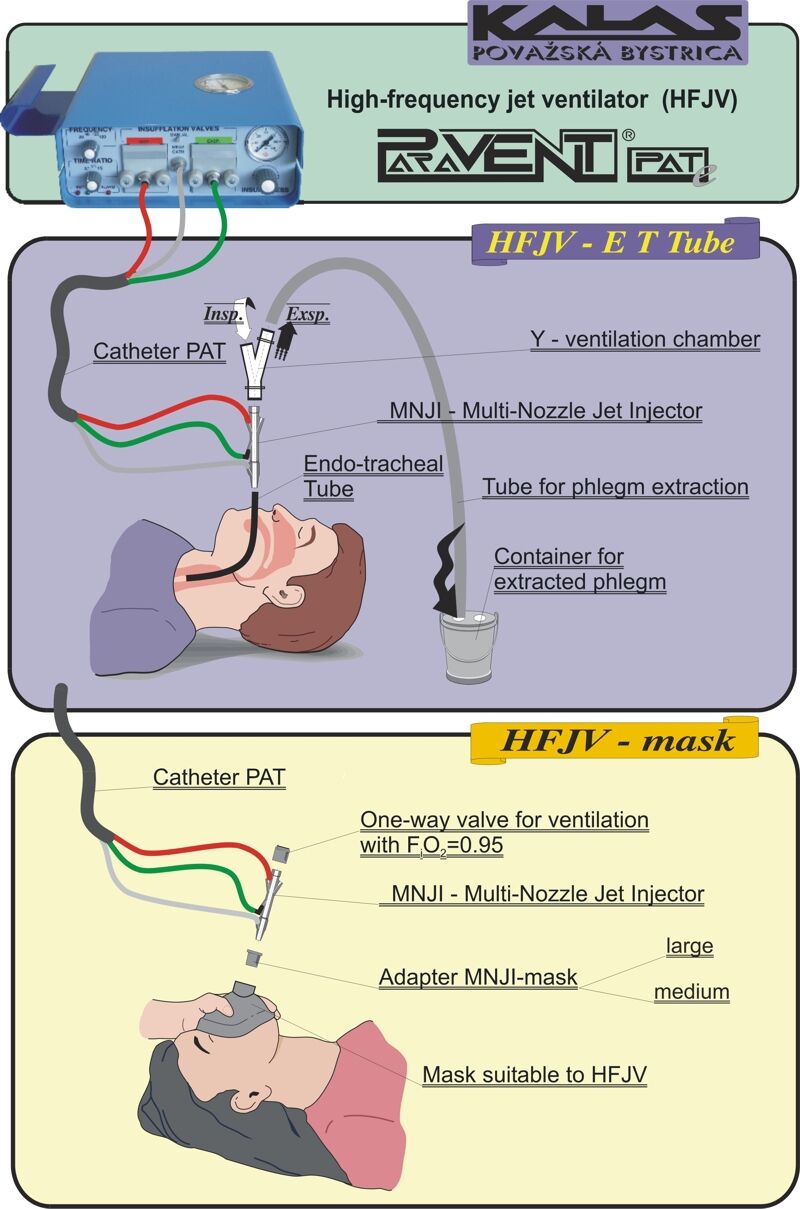
High frequency jet ventilation (HFJV) by PARAVENT ventilators


Brief theoretical background of HFJV:
Critical clinical conditions, when it is not possible to ensure adequate alveolar ventilation with the use of the conventional ventilation or its modifications, require the resolve with the non-conventional ventilation methods.
There is whole scale of clinical situations fulfilling this premise. Such cases are:
- Cases related to decrease of pliability of lungs and decrease of functional residual capacity (lungs fibrosis, aspiration pneumonia, advanced ARDS, obstruction of breathing motions, e.g. while backfilled by soil).
- Bilateral disparity of mechanical characteristics of lungs and thorax (unilateral trauma of lungs and thorax, diaphragmatic hernia, bronchopleural fistula, alar pneumonia).
- Cases with non-uniform mechanical characteristics of the same side of lungs (emphysema bulosum).
- Cases when minimal pressure effects of artificial ventilation of lungs lead to heavy disorder of hemodynamics (cor pulmonale, natal heart defects, hypovolemia).
- Extreme operative act on trachea, bronchi or lungs.
These clinical cases constitute an issue to secure the adequate alveolar ventilation using conventional approach. Cases such as laser treatments in critical extreme inoperative cases of malignant obstructions of main airways, leading to hypoxia or asphyxia, require adequate assurance of ventilation.
The appropriate resolve to the above mentioned cases of requiring ventilation is high-frequency jet ventilation.
High-frequency jet ventilation is such a form of artificial ventilation of lungs, where supraphysiological frequencies of ventilation cycles are used.
Having in mind the above mentioned, high-frequency jet ventilation needs to considered as a supplementary / complementary ventilation to conventional ventilation methods and/or the method that can be applied in the cases when conventional ways are not adequate.
HFJV has certain advantages as well as disadvantages that need to be bear in mind.
Technological advantages:
- Easy use and application (fast switch on and set up of patient)
- Application by non-invasive method (mask) – easy applicability – for paramedics as well
- Long-distance ventilation (up to 10 m by use of special kit) – crashes, disasters in mines, tunnels, blocked patient in a car wrack, etc.
- Ventilation while patient in anaesthesia in examinations in Nuclear magnetic resonant tunnels
- Crisis management (HFJV ensures at least minimal ventilation required for patient to survive even in the cases of compressed thorax and stomach, e.g. buried by ground)
- Trans-tracheal application – as a possibility (crisis management in ‘no intubation – no ventilation’ situations)
- Possibility to use single ventilator for ventilation of patient from weight range from 600 g up to 180 kg
- Possibility of selective bi-bronchial ventilation
- Possibility of urgent ventilation of two patients at the same time with single unit – e.g. in transportation
- Ventilation during bronchoscopics, bronchographics, including extraction of contrast media (filling) at the end of bronchgraphics
- Application of healing aerosol, also during ventilation by mask (nebulizer)
- Use in special applications – ventilation in contaminated space, e.g. by chemicals or gas, etc.
- Catheter ventilation in surgery of airways
- Prevention of aspiration in use of unsealed (uncuffed) endotracheal tube
- Use in emergency vehicles – use by paramedics or doctors in emergency rescue
- Easy and fast application in natural disasters and mass accidents
- Paravent contains limiter of maximal pressure in airways – „total stop“
Physiological and medial advantages:
- Non-interference with spontaneous ventilation
- Programmable movement of extraneous matters (Expulsion and Impulsion mode) – cleaning of airways using HFJV (as a supplement to conventional long-term ventilation)
- Expulsion and Impulsion as a healing process for extraction of aspiration or little extraneous matter (e.g. dust, dirt) and application of pharmaceuticals (lavage)
- Decreases the volume of lung extra-vascular water
- Rising PEEP in ≈ 0,5 kPa = 5 cm H2O
- Lower Pawmax than in conventional ventilation (ca. 30%)
- Low risk of barotrauma
- Application in bronchopleural fistula (lower leak of gases)
- Slight increase of diuresis
- Not necessary to interrupt external cardiac massage (chest compressions) during KPR (for artificial inspirium) – improved transport of O2 and SpO2
- In cases of lung edema, HFJV is sovereign method of ventilation support
Disadvantages of HFJV:
- Higher demand for experience in long application in ICU
- Necessity of proper training of paramedics and doctors (users)
- Issues with humidifying (Paravent is mostly used for short-term high-frequency jet ventilation – without humidifying , or for long-term application by the use of mask)
- Long-term applications – require special wetting system
- In non-adequate application – e.g. with the use of non-original components – risk of barotraumas is high (use only with original components)
- Swift changes of blood gases – hypocapnia
- Possibility of monitoring of MV (minute volume) and VT (tidal volume) (only approximation)
- In non-adequate application of Expulsion or Impulsion modes – flush out of surfactant and creation of yatrogenous ARDS
- Necessity of monitoring Paw (Pt)
- Occasional issues with sealing of mask on patient’s face (e.g. moustache, anodontia, deformations, trauma) in HFJV by mask
Former types of PARAVENT
Pneumatic models: PARAVENT P; PARAVENT PA; PARAVENT PAT
